
Anthony Donskov
Anthony Donskov is the founder of DSC where he serves as the Director of Sport Performance. Donskov holds a Masters Degree in Exercise Science & is the author of Physical Preparation for Ice Hockey.
Compressive Cuff Disease: Training Implications

- Font size: Larger Smaller
- Hits: 4210
- Subscribe to this entry
- Bookmark
The glenohumeral joint is a complex joint affected by the entire Kinetic Chain. It thrives on large amounts of mobility with a sacrifice in stability. At any given time, only 25%-30% of the humeral head is in contact with the gelnoid fossa (1). Sub acromial Impingement (bursal sided) also known as Compressive Cuff disease or external impingement can affect more than just the elderly and working class, it can affect the athletic population as well. Athletes play hard, train hard and push their bodies to the limit on a daily basis. Contact athletes can sustain shoulder injuries through both macro traumatic and micro traumatic events. Shoulder injuries remain the most common site of injury in hockey (1). As strength coaches, programming can also play an important role in preventing cuff issues. A sound knowledge of functional anatomy and appropriate exercise selection can aid in preventing possible pathology.
Sub Aromial What?
The sub acromial space is formed by the: superior aspect of the humeral head below, and the inferior aspect of the acromion, the acromioclavicular joint and the coracoacromial ligament. The subacromial distance is small. The distance was found to be between 9 mm and 10 mm in 175 asymptomatic shoulders. A distance of less than 6mm was considered indicative of rotator cuff disease (2).
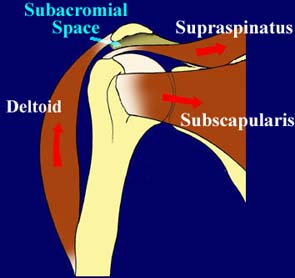
Photo Courtesy of: http://www.zadeh.co.uk/shouldersurgery
What is Compressive Cuff Disease?
Neer describes external impingement as a “mechanical impingement of the supraspinatus and the long head of the biceps tendon underneath the acromial arch. The primary pathologic condition involves a bursal surface lesion (3).”
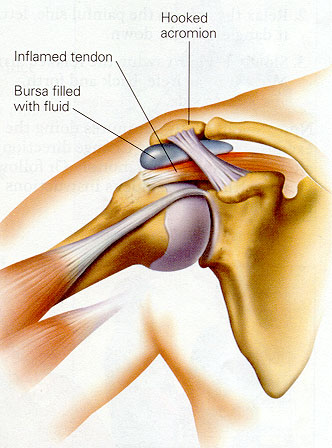
Photo Courtesy of: www.ortho-md.com
Causes:
What causes sub acromial impingement? Donatelli has provided the following list below (4). Factors can be divided into intrinsic and extrinsic. Strength coaches, can appropriate training help in any of these causes?
Intrinsic:
- Vascularity
- Degeneration
- Anatomic/Bony Abnormalities
Extrinsic:
- Muscle Imbalances
- Postural Changes
- Motor Control problems
- Training Errors
As Coaches, we may not be able to change Johnny’s genetic makeup (i.e. Type 1, Type II or Type III aromion), but we can help Johnny prevent muscle Imbalances, motor control issues, and postural changes by implementing effective exercise protocol. These are ALL factors that we control.
Exercise Selection
- Muscle Imbalances/Postural Changes: We need to screen our athletes. FMS and static screening are critical at presenting possible red flags in regards to impingement. Athletes sit as well! Whether in school or driving in the car, this causes musculo skeletal imbalance! This position can decrease both serrauts and lower trap strength. Classic rounded shoulder can bring the acromion process closer to the humeral head and can influence movement of the scapula on the thoracic spine and rib cage (Reinold).

- Open up/Clear the sub acromial space: Again, we can’t alter genetic makeup such as Acromion type, but we can work on musculo skeletal issues. Open up the sub acromial space. How do we do this as coaches?
- Soft tissue work: pec minor, levator scap and upper traps.
- Horizontal Pulling/retraction: DB rows, cable rows, TRX rows
- Attack the Lower Trapezius (upward rotation, depressor of the scap): Face Pulls, Y’s (in the Y, T, W, L circuit), Wall Slides
- Thoracic Spine mobility
- Serratus Anterior Work (protract, upward rotation): Push Up Plus
- Eliminate/Modify Heavy Horizontal Pressing
- Eliminate Overhead Activities: Arthrokinamatic movement dictates that forward flexion of the humerus results in concomitant internal rotation of the humeral head. The result is that the tissue (supraspinatus, biceps tendon) is driven directly under the anteroinferior one third of the acromion (4).
Train the Cuff: The cuff serves to center the humeral head in the gelnoid fossa. According to Reinold the cuff needs strength, balance, support, and endurance. Do NOT work the cuff through pain! Asymptomatic cuff work is key! There has been much debate in the strength and conditioning field regarding effective cuff protocol. It’s important however that our protocol be based more on evidence than just opinion. Below are several cuff exercises based on high EMG activity, muscle recruitment patterns, biomechanical and clinical implications (5). The full table can be found in the Journal of Orthopedic and Sports Physical Therapy, February 2009, Vol. 39.
1.) Supraspinatus: Full Can exercise
2.) Infraspinatus/Teres Minor: Side Lying External Rotation
3.) Serratus: Push Up with plus
As Coaches, it is our job to build effective, safe, RESULTS driven protocol. A sound understanding of functional anatomy is critical in the quest for appropriate exercise selection. It’s one thing to attain imbalance as the result of participating in high impact sports, its quite another attaining them in the weight room! Effective training/exercise selection (and omitting certain exercises) many times can solve problematic issues related to sports and bad posture.
References:
(1) Wilk, K, Reinold, M, Andrews, J, The Athlete’s Shoulder, Churchill Livingstone, 2009.
(2) Peterson, CJ, Redlund-Johnell I: The Subacromial Space in Normal Shoulder Radiographs, Acta Orthop Scand, 55:57, 1984.
(3) Neer, CS, Anterior Acromioplasty for the chronic Impingement Syndrome of the Shoulder, J Bone Joint Surg, 54A:41, 1972.
(4) Donatelli, R, Physical Therapy of The Shoulder: Fourth Edition, Churchill Livingstone, 2004.
(5) Reinold, Escamilla, Wilk, Journal of Orthopedic and Sports Physical Therapy, February 2009, Vol. 39.
Anthony Donskov, MS, CSCS, PES, is a former collegiate and professional hockey player, founder of Donskov Strength and Conditioning, Inc. (www.donskovsc.com) and Head Instructor/Director of Off-Ice Strength and Conditioning for Donskov Hockey Development (www.donskovhockey.com). He can be reached at info@donskovsc.com .
Facebook: http://www.facebook.com/pages/Donskov-Strength-and-Conditioning-Inc/111694352189187
Twitter: http://twitter.com/Donskovsc